In contrast to high levels of low-density lipoprotein cholesterol (LDL-C), where reduction invariably results in clinical benefit (irrespective of the therapy/therapies used), the impact of lowering elevated triglyceride (HTG) levels has been the proverbial “tough nut to crack”. This is largely reflective of TGs status as a biomarker of CVD risk rather than directly causative in the process. Hence, the LDL mantra “lower is better” does not apply to TG, as recently demonstrated in PROMINENT (and other studies). Rather, successful TG lowering treatments must effectively combat the proinflammatory, prothrombotic and pro-oxidative stress associated with the HTG state, as exemplified by icosapent ethyl (IPE) in REDUCE-IT.
Now, a new study offers considerable promise in treating another adverse consequence of HTG, non-alcoholic fatty liver disease (NAFLD); this condition affects 1 in 4 adults worldwide and is projected to increase to 1 in 3 adults by 2030 owing to the continued rise in obesity, Type 2 diabetes and the Metabolic Syndrome. In addition to increased CVD, complications of NAFLD include nonalcoholic steatohepatitis, cirrhosis and liver cancer. While lifestyle therapies resulting in weight reduction of 10% and greater reduce liver fat, no drugs have been approved by the FDA for NAFLD (see the recent American Heart Association Statement led by my colleague, Dr. Bart Duell).
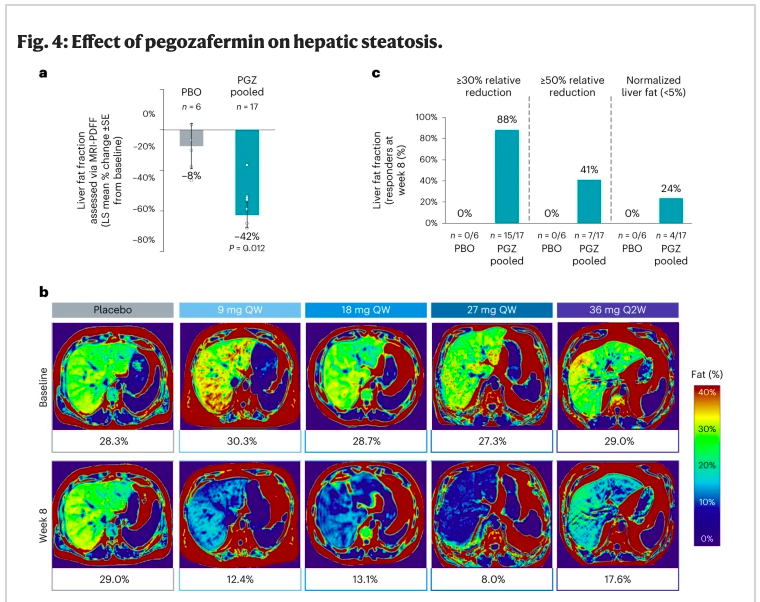
The new study entitled “ENTRIGUE”, examined pegozafermin, an analog of human fibroblast growth factor 21 (FGF21) that upon chemical modification (glycopegylation), permits a longer half-life to suppress de novo lipogenesis and to upregulate fatty acid oxidation, thereby reducing atherogenic lipids/lipoproteins/apolipoproteins. Specifically, among volunteers with severe HTG (500-2,000 mg/dL), weekly (or twice monthly) subcutaneous injections effectively lowered TG (median reduction, 44% compared to placebo) over the 8-week study period; ~80% reduced TG levels to less than 500 mg/dL. Impressively, there was significant reduction in liver fat as quantified by the MRI protein density fat fraction (Figure), with nearly 1 in 4 subjects normalizing their liver fat content during this short timeframe. Equally important was that pegozafermin was well tolerated and no major adverse safety signals were observed.
Michael Miller, MD is a cardiologist and Chief of Medicine at the Corporal Michael J Crescenz VA Medical Center and Professor of Medicine at the Hospital of the University of Pennsylvania. Dr. Miller is Scientific Advisor to Amarin, Inc and 89bio. Prior to his arrival in Philadelphia, he was Professor of Cardiovascular Medicine, Epidemiology and Public Health at the University of Maryland School of Medicine. He is the author of numerous scientific publications and several books, including Heal Your Heart published by Penguin Random House. Check him out on twitter: @mmillermd1
Eskimos: More than half a century ago, Danish researchers Bang and Dyerberg made the astute discovery that Eskimos residing in the Danish territory of Greenland experienced a much lower rate of coronary heart disease than Europeans living in Denmark. As Eskimos consumed high amounts of marine derived omega-3 fatty acids from whale blubber (see photo above), salmon and other fish, they reasoned that the low incidence of myocardial infarction was due to a diet enriched in EPA.
As it turns out, Bang and Dyerberg were right!
With the results of RESPECT-EPA presented at last week’s American Heart Association Scientific Sessions, we now have 4 clinical outcome trials and 2 arteriographic studies pointing in the same direction; simply stated, purified EPA reduces coronary (CAD) events, arteriographic CAD progression and overall cardiovascular risk. Whether studies included patients in primary prevention, secondary prevention or post-ACS, they have generated reproducible results in favor of EPA therapy. In effect, icosapent ethyl the purified form of EPA (marketed in the U.S. as Vascepa, the abbreviated form of Vascular EPA) is currently indicated for patients with high triglycerides (HTG) and CAD or for Type 2 diabetes mellitus (T2DM) with additional CAD risk factors. Now admittedly, RESPECT-EPA had shortcomings that included an open-label design and was underpowered (low event rates/high early withdrawal rates) that would not have garnered significant attention despite the 22% reduction in the primary endpoint (cardiovascular [CV] death, nonfatal myocardial infarction, nonfatal stroke, revascularization and unstable angina requiring hospitalization) (p=0.054) and 27% reduction in the secondary endpoint (CAD events, stroke and mortality) (P=0.03) in Japanese patients with stable CAD assigned to 1.8 grams of EPA daily. However, when RESPECT-EPA is placed within the context of other EPA based studies, there is a clear and consistent trend of improved cardiovascular risk. These results are directionally aligned with the much larger REDUCE-IT trial that used 4 grams daily of highly purified icosapent ethyl (IPE) in men and women with elevated triglycerides and CAD or T2DM that resulted in 25% and 26% reductions in the primary and secondary endpoints, respectively (P< 0.0001; P< 0.0001). In the earlier JELIS study of nearly 20,000 Japanese patients with elevated cholesterol there was an overall 19% reduction in risk of coronary events (p=0.011). Finally in the study by Nosaka and colleagues, assignment to 1.8 grams EPA within 24 hours following percutaneous coronary intervention in the setting of an acute coronary syndrome was associated with a 58% reduction in cardiac events during the 1-year follow-up period (P=0.02). Two angiographic studies CHERRY and EVAPORATE further demonstrated reduced atherosclerotic progression when EPA was added to statin therapy.
Taken together, ALL 6 EPA trials demonstrate improvement in cardiovascular risk.
Fish Oils: In contrast to EPA only studies, the use of fish oils, most commonly a combination of EPA/DHA has not been successful in lowering CV risk. Some have suggested that the daily dose of fish oils used was too low (e.g., 1 gram daily), thereby limiting the rise of circulating EPA levels (that many believe to be the primary basis for the CV benefits) and/or did not test a sufficiently high-risk study population. Nonetheless, the STRENGTH study that used 4 grams of fish oil daily in a high-risk population (HTG and CAD/CAD risk factors) also failed to demonstrate benefit. So why have EPA-only but not EPA/DHA studies improve cardiovascular risk? In this regard, basic science investigations led by my colleague, Dr. Preston Mason has repeatedly shown that DHA offsets favorable actions of EPA (e.g., cellular inflammation, oxidative stress, etc). Does this mean that we should recommend avoiding DHA containing foods? That would not be my recommendation because DHA is 1) vital for brain growth and development (most pronounced during the first 5 years of life) and 2) cardioprotective marine-derived fish contain both EPA/DHA. Thus, while we don’t recommend discontinuing fish consumption, we do recommend purified EPA for our high-risk patients based upon REDUCE-IT inclusion criteria.
Supplements: The most common dietary supplements in the U.S. are fish oil derived. Unfortunately, while the FDA regulates over-the-counter (OTC) drugs, they do not regulate dietary supplements because they are considered food derived products. Not only are fish oil supplements ineffective in reducing cardiovascular risk but they may also contain contaminants such as atherogenic saturated fatty acids. Hence, we do not recommend fish oil supplements and would be very wary of any physician/health care professional who does…even if/especially if they run for Congress!
EPA Deniers: EPA deniers have found a variety of reasons to minimize the fact that purified EPA is highly effective. For one, they point to the open label design (as is customary in Japan) even though both REDUCE-IT and EVAPORATE drew similar/positive conclusions using placebo-controlled groups. Then they will complain that the CV benefit was not due to EPA per se, but rather the mineral oil placebo group that inflicted damage and accelerated CVD events due to LDL-C and hs-CRP elevations. Surely if this were the case, placebo-treated subjects with the highest on-treatment LDL-C or hs-CRP levels would have markedly greater CVD event rates than placebo treated patients without such elevation. However, that line of reasoning was faulty because there were no differences in CVD events irrespective of on-treatment LDL-C or hsCRP in the mineral oil group. In fact, IPE reduced CVD events similarly in these groups. Finally, they will extol that mineral oil caused such severe increases in inflammatory biomarkers that that must have been the reason for the success of REDUCE-IT. Yes, it is true that the mineral oil group evidenced increases in biomarkers that included a 28.9% increase in interleukin-1β (0.06 to 0.08 pg/ml) and 16.2% increase in interleukin-6 (3.27 to 3.76 pg/ml) after 1 year. On the surface this appears to be problematic until the normal range is revealed: interleukin-1β (0.5-12 pg/ml), interleukin-6 (0-43.5 pg/ml). In other words, while there were statistically significant increases in these levels, they were still within the normal range! One is certainly hard-pressed in this case to equate statistical significance with clinical relevance. Hence, the modest effects of mineral oil can in no way account for the sizeable benefits observed in REDUCE-IT, a fact corroborated by the FDA upon issuing their approval indications for IPE in 2019 following unanimous agreement of the scientific advisory team.
Moving forward, let’s direct our focus towards optimizing lipid lowering treatment for our patients at highest CVD risk. The proof is in the pudding when it comes to LDL-C lowering (statins/ezetimibe/PCSK9 inhibitors) and TG lowering (icosapent ethyl) and our patients should receive these therapies as indicated. We await novel therapies currently in clinical trial testing that may provide incremental risk reduction to benefit our patients.
Michael Miller, MD is a cardiologist and Chief of Medicine at the Corporal Michael J Crescenz VA Medical Center and Vice Chair of Medicine at the Hospital of the University of Pennsylvania. Dr. Miller is Scientific Advisor to Amarin, Inc and 89bio. Prior to his arrival in Philadelphia, he was Professor of Cardiovascular Medicine, Epidemiology and Public Health at the University of Maryland School of Medicine. He is the author of numerous scientific publications and several books, including Heal Your Heart published by Penguin Random House. Check him out on twitter: @mmillermd1
I am reminded of my late mentor, Dr. Peter O. Kwiterovich, Jr. who used to say when we published new research findings that “this is another feather in your cap”! Well, this expression could not be truer than what we have been witnessing with icosapent ethyl (IPE), the highly purified omega-3 fatty acid, EPA. First there was the landmark study, REDUCE-IT where IPE reduced the risk of cardiovascular death, heart attack, stroke, bypass/stent placement and rehospitalization for unstable by an astounding 25% in statin treated men and women with high triglycerides and cardiovascular risk. To date, IPE remains the best treatment for patients at similar underlying risk.
Last week, 2 new feathers were added to the IPE cap during presentations at the European Society of Cardiology (ESC), one of medicine’s premier international meetings. The first paper presented by my colleague, Dr. Deepak Bhatt found IPE to reduce the risk of the 2 types of heart attacks (ST and non-ST elevation) by 40% and 27%, respectively. The second feather was the result of another analysis showing that IPE eradicated the excess risk of cardiovascular events attributable to cigarette smoking; the manuscript is published in the European Heart Journal Cardiovascular Pharmacotherapy. For a comprehensive review of other IPE “feathers”, check out the excellent new review by Dr. Prakriti Gabapublished in JCL.
During an ESC presentation, the prominent Danish Professor and Lipid Expert, Dr. Borge Nordestgaard, commented to me that every analysis performed for IPE has shown strikingly positive results. Could the reason for IPEs success be that the compound has unique characteristics that other fatty acids don’t? In fact, my colleague Dr. Preston Mason has performed a number of elegant studies demonstrating that to be the case. Specifically, IPE reduces inflammation and oxidative stress while improving endothelial function.
You certainly don’t have to convince me that IPE acts different fatty acids. Decades ago, we examined the role of purified EPA in human cells and found favorable effects that were not observed with other fatty acids- perhaps a presage of good things to come for IPE.
Michael Miller, MD is a cardiologist and Chief of Medicine at the Corporal Michael J Crescenz VA Medical Center and Vice Chair of Medicine at the Hospital of the University of Pennsylvania. Prior to his arrival in Philadelphia, he was Professor of Cardiovascular Medicine, Epidemiology and Public Health at the University of Maryland School of Medicine. He is the author of numerous scientific publications and several books, including Heal Your Heart published by Penguin Random House. Check him out on twitter: @mmillermd1
I am reminded of my late mentor, Dr. Peter O. Kwiterovich, Jr. who used to say when we published new research findings that “this is another feather in your cap”! Well, this expression could not be truer than what we have been witnessing with icosapent ethyl (IPE), the highly purified omega-3 fatty acid, EPA. First there was the landmark study, REDUCE-IT where IPE reduced the risk of cardiovascular death, heart attack, stroke, bypass/stent placement and rehospitalization for unstable by an astounding 25% in statin treated men and women with high triglycerides and cardiovascular risk. To date, IPE remains the best treatment for patients at similar underlying risk.
Last week, 2 new feathers were added to the IPE cap during presentations at the European Society of Cardiology (ESC), one of medicine’s premier international meetings. The first paper presented by my colleague, Dr. Deepak Bhatt found IPE to reduce the risk of the 2 types of heart attacks (ST and non-ST elevation) by 40% and 27%, respectively. The second feather was the result of another analysis showing that IPE eradicated the excess risk of cardiovascular events attributable to cigarette smoking; the manuscript is published in the European Heart Journal Cardiovascular Pharmacotherapy. For a comprehensive review of other IPE “feathers”, check out the excellent new review by Dr. Prakriti Gabapublished in JCL.
During an ESC presentation, the prominent Danish Professor and Lipid Expert, Dr. Borge Nordestgaard, commented to me that every analysis performed for IPE has shown strikingly positive results. Could the reason for IPEs success be that the compound has unique characteristics that other fatty acids don’t? In fact, my colleague Dr. Preston Mason has performed a number of elegant studies demonstrating that to be the case. Specifically, IPE reduces inflammation and oxidative stress while improving endothelial function.
You certainly don’t have to convince me that IPE acts different fatty acids. Decades ago, we examined the role of purified EPA in human cells and found favorable effects that were not observed with other fatty acids- perhaps a presage of good things to come for IPE.
Michael Miller, MD is a cardiologist and Chief of Medicine at the Corporal Michael J Crescenz VA Medical Center and Vice Chair of Medicine at the Hospital of the University of Pennsylvania. Prior to his arrival in Philadelphia, he was Professor of Cardiovascular Medicine, Epidemiology and Public Health at the University of Maryland School of Medicine. He is the author of numerous scientific publications and several books, including Heal Your Heart published by Penguin Random House. Check him out on twitter: @mmillermd1
It’s hard to believe that not too long ago, revered athletes like Mickey Mantle and even our medical community promoted cigarette smoking! Yet despite the numerous bans, beginning with the cessation of Ads on TV (January 2, 1971), Billboard Ads (April, 1999) and most recently, the FDA’s process to ban JUUL cigarettes, smoking continues to be the #1 most preventable cause of heart disease.
A recent review by the American Heart Association found that compared to non-smokers, tobacco use was associated with the development of heart disease at an earlier age in men and women aged 40-59 years, (5 and 4 years in men and women, respectively). In fact, middle-aged women without a history of heart disease who smoked, doubled their risk of sudden death; in middle-aged men, the risk was increased by 80%. Smoking also increased the risk of stroke in young men and women (less than 40 years of age) and heart failure in middle and older aged men and women.
Today, more than 34 million adults in the United States continue to smoke cigarettes. While these numbers are undoubtedly lower than during the era of incessant tobacco advertising campaigns, the ravaging, long-term health consequences attributable to daily tobacco use persists.
Unfortunately, in the absence of successful smoking cessation efforts, effective therapies to reduce tobacco related cardiac events are highly limited. I can think of 2 (statins and aspirin). Wouldn’t it be nice if there were other treatments available/associated with reduced risk?
Michael Miller, MD is a cardiologist and Chief of Medicine at the Corporal Michael J Crescenz VA Medical Center and Vice Chair of Medicine at the Hospital of the University of Pennsylvania. Prior to his arrival in Philadelphia, he was Professor of Cardiovascular Medicine, Epidemiology and Public Health at the University of Maryland School of Medicine. He is the author of numerous scientific publications and several books, including Heal Your Heart published by Penguin Random House. Check him out on twitter: @mmillermd1
As my 30-plus years as a faculty member at the University of Maryland School of Medicine and Medical Center has drawn to a close, I fondly recall 10 heart-related findings/discoveries and newsworthy events that gained worldwide attention, ending with the first genetically altered pig heart transplanted at UMMS last week. Here they are in no special order.
As we get set to leave Baltimore for Philadelphia, I can’t help but reminisce of the great friendships and memories made in “Charm City”. As a baseball enthusiast, moving to Baltimore in the mid-80s brought me an even greater appreciation of GH (Babe) Ruth, the hometown hero and legendary “Sultan of Swat”. Over the past several decades, my hobby of collecting baseball memorabilia rose to a new depth as I pursued Ruth-related collectibles. Of the 7 baseball cards illustrated, 5 are of the Bambino himself (from the 1933 Goudey and 1948 Leaf set), 1 is of his teammate, Lou Gehrig (1934 Goudey) and on the upper right, is the 1909 T-206 Ty Cobb (green background) acquired from the estate of Babe Ruth’s cousin shortly after my move to Baltimore from Cincinnati.
It is no surprise that we commonly refer to Baltimore as “Small”-timore because there are so many interconnections…in the case of Babe Ruth, I pass by his birth home nearly every day as the University of Maryland Hospital is just a block away. Ironically and many decades earlier, my wife’s family (generations of native Baltimoreans) at one time owned the pub where Babe Ruth’s father was employed (currently the centerfield area of Camden Yards). Even our 13-year-old cockapoo is aptly named “George Herman”!
Listed below are reasons to engage in a hobby that is appealing to you.
Enjoyment of a hobby is associated with an 8-fold lower risk of future cardiovascular events such as heart attack or stroke due to improvement in vascular health.
While the holiday season is jovial and celebratory for the majority of Americans, it can also be a source of despondency and despair for others. This is especially true for those afflicted with seasonal affective disorder or have great fear and anxiety leading to self-imposed travel restrictions in the midst of the COVID pandemic.
Fortunately, as of this writing, the most recent evidence suggests that if you’ve been vaccinated and “boosted”, the latter should be less of an overriding concern.
Nevertheless, as compared to the pre-COVID pandemic era, levels of depression and anxiety have also risen to unforseen heights. With the Holiday Season upon us, presented below is a heart healthy selection of foods/drinks proven to enhance mood and combat/limit depression and make your holiday season a more enjoyable one.
Mushrooms: A new study of nearly 25,000 men and women found that compared to non-consumers, those who ate mushrooms on a regular basis were less likely to experience signs of depression. Mushrooms are an excellent source of ergothioneine (ERGO), an amino acid with antioxidant properties shown (in rodent studies) to alleviate symptoms of depression. Other good food sources of ERGO are beans (black, kidney) and oat bran.
Cranberries: Cranberries are also rich in antioxidants and in the brain protective and anti-inflammatory compound ursolic acid. Ursolic acid not only reduces growth of certain tumors but has also been shown to improve memory and reduce mood disorders, especially anxiety and depression. Try a handful of cranberries or 4 ounces of pure cranberry juice each day to reap the benefits.
It is well established that cardiovascular disease is disproportionately higher in blacks than in whites, Asians and Hispanics. In fact, death from heart disease is 1.7 to 2-fold higher in black men compared to white men 45 years and older. Similarly in women, cardiovascular events are also elevated in blacks compared to whites with an approximate 2.5-fold risk beginning in middle-age (45+ years).
According to the American Heart Association, 7 core health behaviors/risk factors shape the likelihood of developing a heart attack or stroke. They include: blood pressure (BP), body mass index (BMI), cholesterol level, dietary habits, glucose control, physical activity and smoking history. In an otherwise healthy individual, “ideal” cardiovascular health would be defined as optimal core health behaviors/risk factors such as 1) BP less than 120/70; 2) BMI between 18-24.9 kg/m2, 3) LDL cholesterol levels less than 100 mg/dL, 4) a diet low in animal based saturated and trans fats, 5) fasting blood glucose less than 100 mg/dL, 6) being physically active (at least 150 minutes of mild-moderate activity [such as brisk walking at 3-5 mph] per week) and 7) not smoking cigarettes. Unfortunately, less than 1 in 3 adult men/women exhibit ideal cardiovascular health led by Asians (29%) and Whites (19%) while Hispanics and Blacks (14% and 10%) lag well. behind this milestone. For a more comprehensive review on this topic, check out our recent paper led by my colleague, Dr. Penny-Kris Etherton.
Listed below are further insights into the barriers, challenges and opportunities for implementing change to reduce disparities in diet-related heart disease based upon the publication in the Journal of the American Heart Association.
Food deserts are areas that lack access to affordable foods that comprise a healthy diet (e.g., fruits, vegetables, low‐fat milk, whole grains). In Baltimore, high availability of healthy foods was only present in 19% of predominately black neighborhoods compared to 68% of white neighborhoods.
A study conducted in Atlanta found that individuals in food deserts were more likely to be black, less likely to be college graduates, and had lower income compared with individuals in nonfood deserts.
Access to supermarkets stocking affordable healthy foods is associated with greater likelihood of fulfilling healthy dietary recommendations. For each supermarket present in a census tract, the intake of fruits and vegetables rose by 32%.
Large disparities exist in supermarket access in predominately black communities. There are 5 times more supermarkets in census tracts where whites live compared to where blacks reside.
Approximately 3.5% of the US population live in a food swamp, defined by the ratio of fast-food outlets and convenience stores to supermarkets and grocery stores in a given area.
Financial incentives to encourage purchasing of healthy foods and/or disincentives or restrictions on purchasing of unhealthy foods improves diet quality, especially in low‐income groups. A 10% reduction in the price of healthy foods increased consumption by 12%.
An increase in the cost (tax) of unhealthy foods decreased consumption by 6%. This approach reduced intake of sugar‐sweetened beverages (9%), fast food (3%), and other unhealthy beverages (5%).
In our 3rd installment on “Trending Nutrition Controversies” by the American College of Cardiology’s Nutrition Workgroup and led by Dr. Monica Aggarwal, we describe some of the popular dietary-related controversies in 2021. For a link to this publication, press here.
Below are highlights of this review and the evidence for or against the use of these products and development/progression of cardiovascular disease.
Artificial and Non-Nutritive Sweeteners: Whether they contain aspartame (Equal), saccharin (Sweet & Low), sucralose (Splenda) or stevia (Truvia), the artificial sweetener franchise has been stirred into a frenzy as several large studies have linked the frequency of these sweeteners to weight gain, increased risk of Type 2 diabetes and cardiovascular disease. Consequently and until new studies suggest otherwise, we recommend limiting the use of artificial sweeteners. Instead, consider adding unsweetened vanilla/ cocoa extract and/or a cinnamon stick to your morning Java.
Cocoa/Cacao: As a rich source of antioxidants, studies have shown that 1-2 tablespoons of cocoa/cacao daily is associated with 10-15% lower risk of heart disease compared to non-consumers. Minimize use of chocolate-containing products that are highly processed (e.g., sugar and corn syrup) to maintain the benefits.
Soy: Isoflavones (e.g., genistein, daidzein) present in soy are powerful antioxidant and anti-inflammatory mediators. Substitution of soy in place of animal based protein has been associated with reductions in LDL cholesterol (3-5%), systolic blood pressure (5-7 mmHg) and overall improved survival from heart disease and cancer.
Plant-based Meats and Substitutes: Despite the recent hoopla surrounding the alternative meat craze for the plant-based Beyond Burger (mung bean/pea) and Impossible Burger (soy), both products also add saturated fat (coconut oil) and sodium to enhance flavor and texture. While these substitutes may be viewed as “healthier” compared with animal sources of protein, they are viewed as less healthy choices when compared to minimally processed proteins, such as lentils, peas and beans.
Dietary Nitrates: Foods such as beet root, celery and dark green vegetables are high in dietary nitrates. Plant based nitrates promote the production of nitric oxide that in turn improves vascular health, reduces insulin resistance and improves exercise capacity. Supplementation with beetroot juice (high in dietary nitrates) was shown to reduce systolic blood pressure by 8 mmHg (the near equivalence to a single BP medication). After nitrates are converted to nitrites, the antioxidants contained within plant but not animal based products also protect against the formation of carcinogenic nitrite (N-nitroso) compounds.
Grass-Fed versus Grain-Fed Meats: Grass-fed beef has a lower fat content with a more favorable saturated fat profile than consumption of grain-fed meat. However, both grass-fed and grain-fed meats contain trans-fats that promote heart disease and studies to date have not shown differences between the two in cholesterol levels, triglycerides, blood pressure or insulin sensitivity. In case you missed highlights of our 2nd Nutrition Controversy paper press here and see below:
Added Sugars: Individuals should limit added sugar to less than 10% of calories and preferably less than 100 calories daily for women and less than 150 calories daily for men.
Legumes: Consuming 3.5 ounces of legumes (such as beans, chickpeas, lentils and peas) at least 4 times each week is associated with ~15% reduction in the risk of heart disease.
Tea consumption: Daily consumption of any tea is associated with an 8-10% reduced risk of heart attack or stroke.
Kimchi: In a 2-week study in overweight/obese men and women consumed 3 servings (3.5 ounces) of kimchi daily, significant decreases in weight (3.3 lbs), fasting glucose (100to 94 mg/dl), and systolic BP (126 to 121 mm Hg) were observed.
Folic Acid & Vitamin B12: Although folic acid and vitamin B12 supplements lower homocysteine levels, results from large clinical trials studies have failed to demonstrate reduction in cardiovascular events.
Probiotic yogurt: Diabetic patients randomized to probiotic yogurt containing Lactobacillus acidophilus (300 g daily) for 8 weeks experienced a 23% reduction in LDL-C and 15% increase in HDL-C compared with baseline. And for some of the highlights of our 1st Nutrition Controversy paper press here and see below:
Green Leafy Vegetables: For each oz of green leafy vegetables consumed daily, there is a 13% lower risk of developing T2DM.
Southern Foods: A Southern pattern of eating consisting of fried foods, egg dishes, processed meats, and sugar-sweetened drinks is associated with a 50-60% increase in cardiac events over a 6-year period compared to a primarily plant-based pattern.
Cholesterol: For each 300-mg increment in dietary cholesterol (~2 egg yolks), blood cholesterol levels rise 6-7 mg/dL
Blueberries: Consuming ~1 cup of blueberries per day is associated with blood pressure reduction of 7 mm Hg systolic and 5 mm Hg diastolic.
Anthocyanins: A 32% lower risk of a heart attack was observed in those with the highest compared to the lowest quintile of anthocyanin intake (e.g., blueberries and strawberries).
Mixed Nuts: A Mediterranean diet supplemented with a 1 ounce serving of mixed nuts daily for 5 yrs was associated with a 30% lower risk of cardiac events compared with a lower-fat control diet.
Plant-based diet: A study conducted in Tarahumara Indians consuming a plant-based diet (e.g. corn and beans) did not identify a single overweight or hypertensive man during the 4-yr follow-up period.
Vegetable Oils: A study conducted in Costa Rica found that the saturated fat, palm oil used for cooking was associated with 25-30% higher risk of heart disease compared to use of less saturated vegetable oils (soybean and sunflower).









{kind=link}